About M.E.
Myalgic encephalomyelitis (M.E., also known as Chronic Fatigue Syndrome or ME/CFS) is a serious, complex, and debilitating chronic disease. It is a multi-system illness involving brain inflammation, the peripheral nervous system, the immune system, the circulatory system, and cellular metabolism.1 There are over 60 symptoms reported by people with M.E., and symptoms vary both in type and in severity.2
M.E. is characterized by profound fatigue, cognitive dysfunction, sleep abnormalities, dysautonomia (dysfunction of automatic processes, like blood pressure, heart rate or digestion), pain, and other symptoms that are exacerbated by exertion.3 This could include physical, cognitive, emotional, or orthostatic (i.e., being in an upright posture such as standing or sitting) exertion.3
The term “Post Exertional Malaise” (PEM) refers to when someone’s symptoms worsen due to exertion. Exceeding their cellular energy capacity results in a “crash” that can occur up to 24-48 hours after the exertion.3 This has been documented in research using 2-day cardiopulmonary exercise tests and assessing cognitive function after exertion.3

The FUNCAP questionnaire4 is a useful tool for assessing functional capacity in patients with diseases where PEM is present. It doesn’t ask whether the person can do the activity but rather looks at the consequences of doing that activity. The questionnaire provides examples of simple daily tasks, such as having a 5-minute conversation or taking a shower. It then asks patients to assess the impact of that activity on them, and the duration of impact on them. For instance, reading one page could have little impact on one person, but it could cause another person to not be able to do anything else that day.
M.E. affects an estimated 20+ million patients worldwide.1 Research suggests that infection with SARS-CoV-2 (the virus that causes COVID-19) is associated with an increase in the number of M.E. cases, as new incidence cases of M.E. are now 15 times higher than pre-pandemic levels.5 An estimated 70-75% of patients cannot work, and 25% are homebound and/or bedbound.1,6 Full recovery is not common,7 leaving patients ill for years or even decades. Estimates of the economic burden in the USA alone range from $36-51 billion dollars annually (2020 figures).8
Research based on American data has found that M.E. is more underfunded with respect to disease burden than most other debilitating diseases, with M.E. receiving roughly 7% of that commensurate with disease burden.9 M.E. has no widely accepted biomarkers and no FDA-approved treatment.9 The National Institute for Health and Care Excellence’s (NICE; U.K.) Guideline,10 most recently reviewed in 2025, provides information on managing the disease and its symptoms. Treatment options in the NICE Guideline are limited, focusing on energy management (i.e., pacing) and symptom management.
In the midst of statistics, the human cost can be lost. This August 2024 article on the “Forgotten Faces of ME” looks at five people with severe M.E. and their traumatic stories that include being repeatedly subjected to gate-keeping psychological assessments, being subjected to inappropriate medical treatments that resulted in their deterioration, and being unable to access appropriate medical care – even to the point of dying from malnutrition. Whitney Dafoe, one of the people profiled in the article, wrote on his blog: "There are so many improvements needed in the care of ME because prejudice about ME has infected all aspects of our global society, from the general public, to insurance coverage, to health care, to social programs like disability benefits or housing programs to care for those too sick to work. No part of our world in 2024 works to help ME patients. On the contrary, ME patients need to fight, while being often devastatingly sick, for basic rights like access to food, water, and shelter.”11 Unfortunately, stories like this are not uncommon, and the human suffering is enormous.
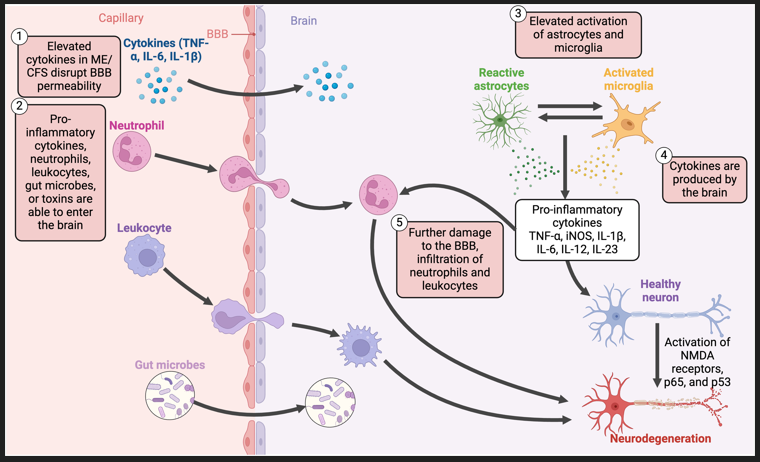
Disruption of the blood-brain barrier, the translocation of pro-inflammatory cytokines, and chronic activation of various non-neuronal cells contribute to neuroinflammatory mechanisms in ME/CFS.
Arron HE, Marsh BD, Kell DB, Khan MA, Jaeger BR and Pretorius E (2024) Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: the biology of a neglected disease. Front. Immunol. 15:1386607. doi: 10.3389/fimmu.2024.1386607
While more funding and effective treatments remain urgently needed, there has been significant and meaningful progress. In the early 2020s, M.E. research slowly gained momentum as outstanding researchers explored key areas of investigation such as biomarkers, neuroinflammation, and microclots. Large-scale studies such as DecodeME, investigating genetic factors, and BioQuest, identifying biomarkers of disease subsets, have advanced our understanding of M.E. Evidence-based clinical care guidelines were developed that valued lived experience alongside clinical expertise and research, and noted specific harmful treatments that were contraindicated. Creative and impactful advocacy campaigns attracted increasing national and international coverage, raising public awareness of M.E. and long covid. The phenomenal work of dedicated researchers, community scientists, clinicians, advocates, patients, caregivers, and organizations is advancing the scientific and public understanding of this disease, and is making important headway towards long-overdue recognition and treatment.